
2016 , Vol. 10 >Issue 02: 97 - 100
DOI: https://doi.org/10.3877/cma.j.issn.1674-0807.2016.02.007
慢性乳腺炎临床特点及其治疗
Copy editor: 刘军兰
收稿日期: 2016-03-01
网络出版日期: 2024-12-07
版权
Clinical characteristics and treatment of chronic mastitis
Received date: 2016-03-01
Online published: 2024-12-07
Copyright
目的
分析不同病理类型慢性乳腺炎的临床特点及其手术方式。
方法
本研究纳入2003年2月至2015年11月于第三军医大学西南医院乳腺外科住院治疗的慢性乳腺炎患者259 例,并根据病理结果分为浆细胞性乳腺炎(plasma cell mastitis,PCM)组(n = 111)和肉芽肿性乳腺炎(granulomatous mastitis, GM)组(n=148)。 分析其病例资料,比较两组的临床特征及手术方式, 并根据随访结果分析其复发情况。年龄、住院时间等计量资料比较采用独立样本t 检验、秩和检验,其余指标采用χ2 检验,Kaplan-Meier 生存曲线分析复发间隔时间。
结果
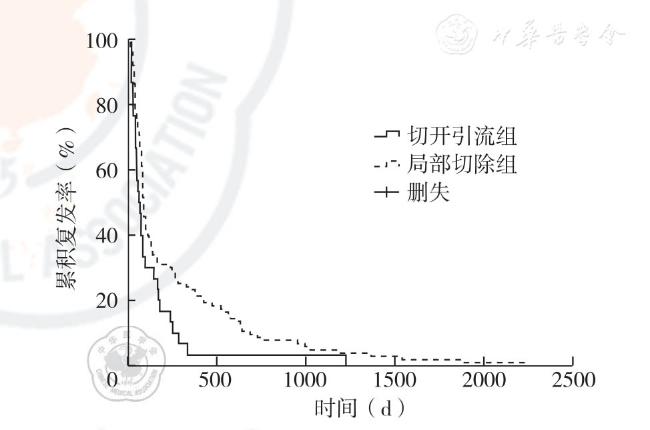
PCM 组发病年龄为(30.1±6.9)岁,低于GM 组(32.7±7.8)岁(t=2.81,P=0.005),两组发病年龄分布的差异有统计学意义(χ2=10.36,P=0.006),患者发病主要集中在26 ~35 岁。 以单纯肿块型为主要临床表现的患者分别占GM 组和PCM组的72.3%和52.3%,两组主要临床表现类型分布差异有统计学意义(χ2=13.68,P=0.003)。 GM 组和PCM 组病变部位距离乳头2cm 以内的例数分别为105 例(70.9%, 105/148)和93 例(83.8%,93/111),差异有统计学意义(χ2 = 5.80,P = 0.016)。 GM 组患者无乳头内陷者101 例(68.2%,101/148),PCM 组无乳头内陷者为54 例(48.7%,54/111),差异有统计学意义(χ2=10.13,P=0.001)。与GM 组比较,PCM 组院外治疗抗生素及激素使用史的患者更多(χ2=4.87,P=0.027),病变位置及手术次数构成差异无统计学意义(χ2=7.32,P=0.198;χ2=3.95,P=0.139)。 全部患者中,接受切开引流38 例、包块或局部切除186 例、全乳切除35 例, 复发率分别为78.9%(30/38)、55.4%(103/186)和0,差异有统计学意义(χ2=49.74, P<0.001),其中切开引流组复发率高于包块或局部切除组(χ2=7.27,P=0.007)。 切开引流组和包块局部切除组复发间隔时间分别为66.0 d、92.0 d,差异有统计学意义(χ2=4.90, P=0.030)。
结论
PCM 患者发病年龄小于GM, 两者均以单纯肿块型为主要临床表现,PCM 病变多位于距离乳头2 cm 以内。 包块或局部切除法治疗优于切开引流法治疗。
潘沁汶 , 魏宏屹 , 苑龙 , 姜军 . 慢性乳腺炎临床特点及其治疗[J]. 中华乳腺病杂志(电子版), 2016 , 10(02) : 97 -100 . DOI: 10.3877/cma.j.issn.1674-0807.2016.02.007
Objective
To investigate clinical characteristics and surgical options for different pathological types of chronic mastitis.
Methods
The study included 259 hospitalized patients with chronic mastitis in Department of Breast Surgery, Southwest Hospital, from February 2003 to November 2015.According to pathological findings, they were divided into plasma cell mastitis (PCM) group (n=111) and granulomatous mastitis (GM) group (n=148). Clinical data were compared between two groups, including clinical features and surgical options, and the follow-up data were analyzed to compare the recurrence.Measurement data including age, hospital stay were processed using independent sample t test and rank sum test, count data were processed using chi-square test and Kaplan-Meier survival curve was used to analyze the recurrence.
Results
The average onset age was (30.1 ± 6.9) years in PCM group, significantly lower than(32.7 ± 7.8) years in GM group (t=2.81, P=0.005). The distribution of onset age showed a statistical difference between groups (χ2=10.36, P=0.006). Most of chronic mastitis patients were 26 to 35 years old.The patients with single mass as the main clinical manifestations accounted for 72.3% in GM group and 52.3% in PCM group respectively. The main clinical manifestations between two groups were significantly different (χ2=13.68, P=0.003). There were 105 patients (70.9%,105/148) with the distance from lesion to nipple≤2 cm in GM group, 93 (83.8%, 93/111) in PCM group, and the difference was statistically significant (χ2=5.80, P=0.016). There were 101 patients without inverted nipple (68.2%,101/148) in GM group,54 (48.7%,54/111) in PCM group, suggesting a statistical difference (χ2=10.13, P=0.001).More PCM patients had more previous use of antibiotic and hormonal drugs than GM patients did (χ2=4.87,P=0.027). There was no significant difference between two groups in lesion location and operation frequency distribution (χ2=7.32, P=0.198; χ2 =3.95, P=0.139). In all patients, 38 cases received incision and drainage, 186 received mass or local resection and 35 received mastectomy, and the recurrence rate was 78.9% (30/38), 55.4% (103/186) and 0 respectively, indicating a significant difference in patients receiving different operations (χ2 =49.74, P <0.001). The recurrence rate in patients with drainage was significantly higher than that in patients with mass or local resection(χ2=7.27,P=0.007).The interval from operation to recurrence was 66.0 d in patients receiving incision and drainage, 92.0 d in patients receiving mass or local resection, indicating a significant difference (χ2=4.90, P=0.030).
Conclusions
PCM has lower onset age than GM, while both have single mass as main clinical manifestation. PCM lesions are mostly located within 2 cm from the nipple. The mass or local resection is superior to drainage in chronic mastitis.
Key words: Mastitis; Drainage; Mastectomy; Recurrence
 ±s 表示,采用独立样本t 检验、秩和检验比较,计数资料采用χ2 检验,Kaplan-Meier 生存曲线分析复发间隔时间。 P<0.050 为差异有统计学意义。
±s 表示,采用独立样本t 检验、秩和检验比较,计数资料采用χ2 检验,Kaplan-Meier 生存曲线分析复发间隔时间。 P<0.050 为差异有统计学意义。表1 两组慢性乳腺炎患者发病年龄分布(例) |
| 组别 | 例数 | <25岁 | 26-35岁 | ≥36岁 |
|---|---|---|---|---|
| GM组 | 148 | 19 | 87 | 42 |
| PCM组 | 111 | 32 | 55 | 24 |
| χ2值 | 10.36 | |||
| P值 | 0.006 | |||
表2 两组慢性乳腺炎患者临床表现比较(例) |
| 组别 | 例数 | 单纯肿块型 | 脓肿型 | 混合型 | 窦道型 |
|---|---|---|---|---|---|
| GM组 | 148 | 107 | 12 | 27 | 2 |
| PCM组 | 111 | 58 | 16 | 37 | 0 |
| χ2值 | 13.68 | ||||
| P值 | 0.003 | ||||
表3 两组慢性乳腺炎患者手术次数比较 |
| 组别 | 例数 | 手术次数 | ||
|---|---|---|---|---|
| 首次手术 | 2次手术 | 3次及以上 | ||
| GM组 | 148 | 56 | 65 | 27 |
| PCM组 | 111 | 29 | 58 | 24 |
| χ2值 | 3.95 | |||
| P值 | 0.139 | |||
| [1] |
王颀.应重视非哺乳期乳腺炎的诊治和研究[J/CD]. 中华乳腺病杂志:电子版,2013,7(3):154-156.
|
| [2] |
Cutler M. Plasma-cell mastitis: report of a case with bilateral involvement[J]. Br Med J,1949,1(4593):94-96.
|
| [3] |
Kessler E, Wolloch Y. Granulomatous mastitis: a lesion clinically simulating carcinoma[J]. Am J Clin Pathol,1972,58(6):642-646.
|
| [4] |
Kok KY, Telisinghe PU. Granulomatous mastitis: presentation,treatment and outcome in 43 patients[J]. Surgeon,2010,8(4):197-201.
|
| [5] |
Ocal K, Dag A, Turkmenoglu O, et al. Granulomatous mastitis:clinical, pathological features, and management[J]. Breast J, 2010,16(2):176-182.
|
| [6] |
Kim J, Tymms KE, Buckingham JM. Methotrexate in the management of granulomatous mastitis[J]. ANZ J Surg,2003,73(4):247-249.
|
| [7] |
Azlina AF, Ariza Z, Arni T, et al. Chronic granulomatous mastitis:diagnostic and therapeutic considerations[J]. World J Surg, 2003,27(5):515-518.
|
| [8] |
Nakamura T, Yoshioka K, Miyashita T, et al. Granulomatous mastitis complicated by arthralgia and erythema nodosum successfully treated with prednisolone and methotrexate[J]. Intern Med, 2012, 51(20):2957-2960.
|
| [9] |
Kieffer P, Dukic R, Hueber M, et al. A young woman with granulomatous mastitis: a corynebacteria may be involved in the pathogenesis of these disease[J]. Rev Med Interne, 2006, 27(7):550-554.
|
| [10] |
Rahal RM, de Freitas-Júnior R, Paulinelli RR. Risk factors for duct ectasia[J]. Breast J,2005,11(4):262-265.
|
| [11] |
苏莉.浆细胞性乳腺炎CD3、CD20、CDs8 表达及其免疫机制研究[D].银川:宁夏医科大学,2009:4-36.
|
| [12] |
Dong Y,Yu JJ,Shibahara Y,et al. Intercellular adhesion molecule 1/2 and E-selectin in plasma cell mastitis: immunohistochemical study of 35 cases[J]. Hum Pathol,2014,45(3):606-610.
|
| [13] |
Tuli R, O'Hara BJ, Hines J, et al. Idiopathic granulomatous mastitis masquerading as carcinoma of the breast: a case report and review of the literature[J]. Int Semin Surg Oncol,2007,4:21.
|
| [14] |
顾斐,邹强. 非哺乳期乳腺炎120 例诊治分析〔J〕. 中国临床医学,2008,15 (2):275-276.
|
| [15] |
Pereira FA, Mudgil AV, Macias ES, et al. Idiopathic granulomatous lobular mastitis[J]. Int J Dermatol,2012,51(2):142-151.
|
| [16] |
Ming J, Meng G, Yuan Q, et al. Clinical characteristics and surgical modality of plasma cell mastitis: analysis of 91 cases[J]. Am Surg,2013,79(1):54-60.
|
| [17] |
Ammari FF, Yaghan RJ, Omari AK. Periductal mastitis. Clinical characteristics and outcome[J]. Saudi Med J,2002,23(7):819-822.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}