
2013 , Vol. 07 >Issue 02: 91 - 96
DOI: https://doi.org/10.3877/cma. j. issn.1674-0807.2013.02.004
Ki67、增殖细胞核抗原在不同分子分型乳腺癌组织中的表达及意义
Copy editor: 刘军兰
收稿日期: 2012-10-29
网络出版日期: 2024-12-07
版权
Expression of Ki67 and proliferating cell nuclear antigen in different subtypes of breast cancer and their clinical significance
Received date: 2012-10-29
Online published: 2024-12-07
Copyright
目的
探讨Ki67、增殖细胞核抗原(PCNA)在不同分子类型乳腺癌组织中的表达及临床意义。
方法
采用免疫组化法检测251 例乳腺癌组织中Ki67、PCNA 的表达情况,采用kruskal-wallis 秩和检验分析Ki67、PCNA 在不同分子类型乳腺癌组织中的表达差异;采用Spearman 相关分析法,分析不同分子类型中Ki67 与PCNA 表达的相关性及其分别与原发肿瘤直径、腋窝淋巴结转移及病理组织学分级的相关性;采用生存分析法,分析Ki67、PCNA 对乳腺癌预后的意义。
结果
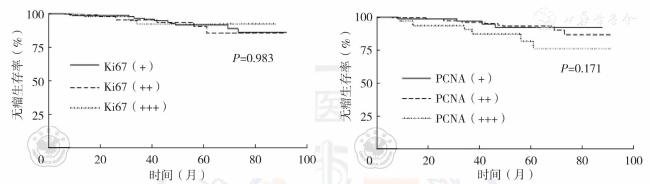
Luminal 型、HER-2 型及三阴性乳腺癌组织中Ki67、PCNA 表达强度差异均无统计学意义(χ2 =3.722,P=0.155;χ2 =5.135,P=0.077)。 Ki67 与PCNA 总体呈正相关(rs=0.348,P=0.000),在Luminal 型中呈正相关(rs=0.467, P=0.000),而在HER-2 型、三阴性乳腺癌中无相关性(P>0.05)。 Ki67 表达强度与原发肿瘤直径、腋窝淋巴结转移及组织学分级在Luminal 型乳腺癌呈正相关性(rs=0.180,P=0.017; rs=0.236,P=0.002; rs=0.156,P=0.039),而在HER-2 型及三阴性乳腺癌中无相关性(P>0.05)。 PCNA 表达强度与Luminal 型乳腺癌的腋窝淋巴结转移呈正相关性(rs=0.166,P=0.028),与HER-2 型乳腺癌的原发肿瘤直径呈负相关性(rs=-0.342,P=0.020),与其他病理因素均无相关性(P>0.05)。 单因素生存分析显示腋窝淋巴结转移、组织学分级对乳腺癌患者无瘤生存有影响(HR=4.431,95%CI:1.787 ~10.984; HR=2.492,95%CI:1.032 ~6.018),亚组分析显示腋窝淋巴结、PCNA 对Luminal 型乳腺癌患者无瘤生存有影响(HR=3.930,95%CI:1.343 ~11.501;HR=2.401,95%CI:1.044 ~5.524)。 多因素COX 回归分析显示腋窝淋巴结转移是总体和Luminal 型乳腺癌患者预后的独立影响因素(HR=3.780, 95%CI:1.461 ~9.775;HR=3.403,95%CI:1.150 ~10.075)。
结论
Ki67 和PCNA 对评估Luminal 型乳腺癌预后有一定指导意义,而对HER-2 型和三阴性乳腺癌预后无明显影响。
董欢 , 林燕苹 , 应学翔 , 何萍青 . Ki67、增殖细胞核抗原在不同分子分型乳腺癌组织中的表达及意义[J]. 中华乳腺病杂志(电子版), 2013 , 07(02) : 91 -96 . DOI: 10.3877/cma. j. issn.1674-0807.2013.02.004
Objective
To investigate the expression of Ki67 and proliferating cell nuclear antigen(PCNA) in three different subtypes of breast cancer and their clinical significance.
Methods
Immunohistochemistry was used to detect the expression of Ki67 and PCNA in tissue samples from 251 breast cancer patients. kruskal-wallis rank sum test was used to analyze the expression difference of Ki67 and PCNA in different subtypes, Spearman rank test for the correlation of their expressions, and the correlation with primary tumor diameter, axillary lymph node metastasis and pathological classification, respectively. Meanwhile, the survival analysis was conducted to display the prognostic value of Ki67 and PCNA expression.
Results
The expressions of Ki67 and PCNA were not significantly different among the three subtypes of breast cancer(luminal,HER-2 and triple negative) (χ2 =3.722,P=0.155;χ2 =5.135,P=0.077). There was a positive correlation between Ki67 and PCNA expressions in general(rs=0.348,P<0.001)and in luminal subtype(rs=0.467, P<0.001), but no correlation was observed in other subtypes(P>0.05). In luminal subtype, the expression of Ki67 was positively correlated with primary tumor diameter, axillary lymph node status and histological grade (rs=0.180,P=0.017;rs=0.236,P=0.002;rs=0.156,P=0.039, respectively), and no correlation was showed in HER-2 and triple-negative subtypes(P >0.05). We also observed the positive correlation between PCNA expression and axillary lymph node status in luminal subtype, a negative correlation with primary tumor diameter in HER-2 subtype (rs = -0.342, P=0.020), but no correlations with other pathological factors were found (P >0.05). Univariate analysis showed axillary lymph node metastasis and nuclear grade had influence on tumor-free survival of breast cancer patients (HR=4.431, 95%CI: 1.787 to 10.984; HR= 2.492, 95% CI: 1.032 to 6.018). The subgroup analysis displayed axillary lymph node metastasis and PCNA had effects on tumor-free survival in luminal subtype (HR=3.930, 95%CI: 1.343 to 11.501; HR=2.401, 95% CI: 1.044 to 5.524). Multivariate COX analysis showed axillary lymph node metastasis was an independent prognostic factor in general and luminal subtype breast cancer patients (HR=3.780,95%CI:1.461 to 9.775; HR=3.403,95%CI:1.150 to 10.075).
Conclusion
Ki67 and PCNA can indicate the poor prognosis of luminal subtype breast cancer patients to a certain extent, but have no influence on HER-2 and triple negative subtypes.
表1 251 例乳腺癌患者的临床及病理资料 |
| 变量 | 例数(%) |
|---|---|
| 年龄 | |
| ≤50岁 | 85(34) |
| >50岁 | 166(66) |
| 组织学分级 | |
| Ⅰ、Ⅱ | 143(57) |
| Ⅲ | 108(43) |
| 肿瘤直径 | |
| ≤2cm | 127(51) |
| >2cm | 124(49) |
| 腋窝淋巴结 | |
| 阴性 | 167(67) |
| 阳性 | 84(33) |
| Ki67 | |
| + | 120(48) |
| ++ | 87(35) |
| +++ | 44(17) |
| PCNA | |
| + | 63(25) |
| ++ | 156(62) |
| +++ | 32(13) |
| 分子分型 | |
| Luminal型 | 175(70) |
| HER-2型 | 46(18) |
| 三阴性乳腺癌 | 30(12) |
表2 Ki67、PCNA 表达与Luminal 型乳腺癌临床病理因素的关系 |
| 病理因素 | Ki67表达(例) | rs值 | P值 | PCNA表达(例) | rs值 | P值 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| + | ++ | +++ | + | ++ | +++ | |||||
| PTD | ||||||||||
| ≤2cm | 56 | 25 | 12 | 0.180 | 0.017 | 24 | 57 | 12 | 0.095 | 0.213 |
| >2cm | 35 | 29 | 18 | 16 | 51 | 15 | ||||
| ALN | ||||||||||
| - | 67 | 34 | 12 | 0.236 | 0.002 | 30 | 70 | 13 | 0.166 | 0.028 |
| + | 24 | 20 | 18 | 10 | 38 | 14 | ||||
| 组织学分级 | ||||||||||
| Ⅰ、Ⅱ | 57 | 32 | 11 | 0.156 | 0.039 | 28 | 56 | 16 | 0.090 | 0.235 |
| Ⅲ | 34 | 22 | 19 | 12 | 52 | 11 | ||||
表3 单因素生存分析结果 |
| 影响因素 | 回归系数 | 统计量(Z值) | P值 | HR(95%CI) |
|---|---|---|---|---|
| 总体 | ||||
| 年龄(≤50岁/>50岁) | 0.567 | 1.11 | 0.269 | 1.763(0.646~4.815) |
| 肿瘤直径(>2cm/≤2cm) | 0.806 | 1.74 | 0.082 | 2.238(0.903~5.548) |
| 腋窝淋巴结(+/-) | 1.489 | 3.21 | 0.001 | 4.431(1.787~10.984) |
| 组织学分级(Ⅲ/Ⅰ、Ⅱ) | 0.913 | 2.03 | 0.042 | 2.492(1.032~6.018) |
| Ki67(+++/+、++) | 0.023 | 0.08 | 0.938 | 1.023(0.569~1.841) |
| PCNA(+++/+、++) | 0.526 | 1.48 | 0.140 | 1.691(0.842~3.397) |
| Luminal型(亚组) | ||||
| 年龄(≤50岁/>50岁) | 0.440 | 0.75 | 0.452 | 1.552(0.494~4.876) |
| 肿瘤直径(>2cm/≤2cm) | 0.634 | 1.20 | 0.229 | 1.886(0.670~5.303) |
| 腋窝淋巴结(+/-) | 1.369 | 2.50 | 0.012 | 3.930(1.343~11.501) |
| 组织学分级(Ⅲ/Ⅰ、Ⅱ) | 0.841 | 1.59 | 0.111 | 2.320(0.824~6.526) |
| Ki67(+++/++/+) | 0.262 | 0.79 | 0.430 | 1.299(0.679~2.487) |
| PCNA(+++/++/+) | 0.876 | 2.06 | 0.039 | 2.401(1.044~5.524) |
表4 多因素生存分析结果 |
| 影响因素 | 回归系数 | 统计量(Z值) | P值 | HR(95%CI) |
|---|---|---|---|---|
| 总体 | ||||
| 腋窝淋巴结(+/-) | 1.330 | 2.74 | 0.006 | 3.780(1.461~9.775) |
| 组织学分级(Ⅲ/Ⅰ、Ⅱ) | 0.513 | 1.09 | 0.276 | 1.670(0.664~4.202) |
| Luminal型(亚组) | ||||
| 腋窝淋巴结(+/-) | 1.225 | 2.21 | 0.027 | 3.403(1.150~10.075) |
| PCNA(+++/++/+) | 0.729 | 1.68 | 0.092 | 2.073(0.887~4.842) |
| [1] |
赵尔扬,方明,施磊,等. 增殖细胞核抗原和Ki67 在口腔癌浸润前沿表达及意义[J]. 口腔医学研究, 2008, 24(5):495-497.
|
| [2] |
苗龙,黄晓俊. Ki67 和PCNA 在胃癌中的表达及其临床诊断价值[J]. 临床内科杂志,2011,28(2):95-97.
|
| [3] |
Calascibetta A, Cabibi D, Rausa L, et al. Difference in Ki67 and thymidylate synthase expression in primary tumour compared with metastatic nodes in breast cancer patients[J].Nucleosides Nucleotides Nucleic Acids, 2006, 25 (9/11):1193-1196.
|
| [4] |
Masuda H, Masuda N,Kodama Y,et al. Predictive factors for the effectiveness of neoadjuvant chemotherapy and prognosis in triple-negative breast cancer patients[J]. Cancer Chemother Pharmacol,2011,67(4):911-917.
|
| [5] |
Faneyte IF, Schrama JG, Peterse JL,et al. Breast cancer response to neoadjuvant chemotherapy: predictive markers and relation with outcome[J]. Br J Cancer,2003,88(3):406-412.
|
| [6] |
Zhao H, Ho PC, Lo YH, et al. Interaction of proliferation cell nuclear antigen (PCNA) with c-Abl in cell proliferation and response to DNA damages in breast cancer[J]. PLoS One,2012,7(1): e29416.
|
| [7] |
NCCN 乳腺癌专家组. NCCN 乳腺癌临床实践指南(中国版)[S]. 北京:NCCN 乳腺癌临床实践指南(中国版)讨论组,2011.
|
| [8] |
Aleskandarany MA, Green AR, Benhasouna AA, et al.Prognostic value of proliferation assay in the luminal, HER2-positive, and triple-negative biologic classes of breast cancer[J]. Breast Cancer Res,2012,14(1): R3.
|
| [9] |
Sorlie T, Perou CM, Tibshirani R, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications[J]. Proc Natl Acad Sci USA,2001,98(19):10 869-10 874.
|
| [10] |
Cheang MC, Voduc D, Bajdik C, et al. Basal-like breast cancer defined by five biomarkers has superior prognostic value than triple-negative phenotype[J]. Clin Cancer Res, 2008,14(5): 1368-1376.
|
| [11] |
Gerdes J, Schwab U, Lemke H, et al. Production of a mouse monoclonal antibody reactive with a human nuclear antigen associated with cell proliferation[J]. Int J Cancer,1983,31(1):13-20.
|
| [12] |
MacCallum DE, Hall PA. The location of pKi67 in the outer dense fibrillary compartment of the nucleolus points to a role in ribosome biogenesis during the cell division cycle [J]. J Pathol,2000,190(5):537-544.
|
| [13] |
Ogata K, Kurki P, Celis JE, et al. Monoclonal antibodies to a nuclear protein ( PCNA/cyclin ) associated with DNA replication[J]. Exp Cell Res,1987,168(2):475-486.
|
| [14] |
Surowiak P, Pudelko M, Maciejczyk A, et al. The relationship of the expression of proliferetron--related antigens Ki67 and PCNA in the cells of ductal breast cancer with the differentiation grade[J]. Ginekol Pol,2005,76(1):9-14.
|
| [15] |
Jalava P, Kuopio T, Juntti-Patinen L, et al. Ki67 immunohistochemistry: a valuable marker in prognostication but with a risk of misclassification: proliferation subgroups formed based on Ki67 immunoreactivity and standardized mitotic index[J]. Histopathology,2006,48(6):674-682.
|
| [16] |
祝玉祥,章佳,邵稳喜,等. ki67 在三阴性乳腺癌组织中的表达及意义[J]. 中国现代普通外科进展, 2010,13(9):679-680,697.
|
| [17] |
沈三弟,陈卓荣,黄湛,等. Ki67 在不同分子类型乳腺癌组织中的表达及意义[J]. 实用癌症杂志,2012,27(3):247-249.
|
| [18] |
Georgescu R, Coros MF, Stolnicu S, et al. Prognostic factors in breast cancer[J]. Rev Med Chir Soc Med Nat Iasi, 2012,116(1):262-267.
|
| [19] |
Gohari MR, Khodabakhshi R, Shahidi J, et al. The impact of multiple recurrences in disease-free survival of breast cancer:an extended Cox model[J]. Tumori,2012,98(4):428-433.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}