
2012 , Vol. 06 >Issue 02: 147 - 152
DOI: https://doi.org/10.3877/cma. j. issn.1674-0807.2012.02.004
超声BI-RADS 3 级乳腺不可扪及病变的微创活组织检查
Copy editor: 刘军兰
收稿日期: 2012-01-18
网络出版日期: 2024-12-07
基金资助
广东省医学科研基金资助项目(No.A2006095)
版权
Ultrasound-guided vacuum-assisted biopsy for BI-RADS grade 3 nonpalpable breast lesions
Received date: 2012-01-18
Online published: 2024-12-07
Copyright
目的
探讨超声检查BI-RADS 3 级的乳腺不可扪及病变(nonpalpable breast lesion, NPBL)微创活组织检查(活检)的临床价值。
方法
回顾性分析2007 年1月至2010 年12 月在本院接受微创活检、超声BI-RADS 3 级的542 例NPBL 病例的临床、影像及病理资料,采用卡方检验比较即时活检组(首次超声诊断后3 个月之内活检)与随访活检组(随访6 个月后活检)发现恶性病变的概率以及两组恶性肿瘤情况的差异。
结果
全组542 例病例,病理确诊恶性病变5 例,总体恶性率为0.92%(5/542);50 ~59 岁患者的恶性率为9.68%(3/31),明显高于其他年龄组(20 ~29 岁组0,30 ~39 岁组0.40%,40 ~49 岁组0.57%,60 ~71 岁组0)。 即时活检组中恶性病变4例,恶性率为0.91%(4/435);随访活检组中恶性病变1 例,恶性率为0.93%(1/107),两者差异无统计学意义(P>0.05),且两组发现的恶性肿瘤的病灶大小,TNM 分期相似。
结论
超声检查BI-RADS 3 级的NPBL 恶性率低,随访活检是安全的。 但对于年龄50 岁及以上,超声评估为BI-RADS 3 级的患者需提高警惕,建议积极进行活检。
吴玲 , 王颀 , 连臻强 , 张安秦 , 李文萍 , 马小燕 , 郜红艺 . 超声BI-RADS 3 级乳腺不可扪及病变的微创活组织检查[J]. 中华乳腺病杂志(电子版), 2012 , 06(02) : 147 -152 . DOI: 10.3877/cma. j. issn.1674-0807.2012.02.004
Objective
To investigate the clinical significance of ultrasound-guided vacuum-assisted biopsy for BI-RADS grade 3 nonpalpable breast lesion (NPBL).
Methods
The clinical, imaging and histopathologic data of 542 cases of NPBL classified as grade 3 in BI-RADS and undergoing vacuum-assisted ultrasound-guided biopsy in our hospital from January 2007 to December 2010 were retrospectively analyzed. The patients were divided into group A (biopsy within 3 months after first ultrasonic diagnosis) and group B (biopsy after 6-month follow-up). The malignant rates and tumor stage were compared between the two groups.
Results
In all 542 patients, 5 were proved to be malignant (0.92%). The malignant rate in the age group of 50-59 years was 9.68%(3/31), which was significantly higher than that in other age groups (20-29 years, 0; 30-39 years, 0.40%;40-49 years,0.57%;60-71 years,0). Four patients presented malignant lesion (0.91%) in group A,1 patient (0.93%) in group B, and no significant difference was showed between the two groups(P>0.05). Malignant cases in two groups showed similar tumor size and TNM stage.
Conclusions
NPBL of BI-RADS grade 3 has low malignant rate and biopsy in follow-up is safe for those patients. However, more attention should be paid for the patients ≥50 years with BI-RADS grade 3 NPBL and clinical biopsy is recommended.
Key words: breast neoplasms; ultrasonography; biopsy; nonpalpable breast lesions
表1 BI-RADS 3 级的NPBL 不同年龄组的病理结果 |
| 年龄 | 例数 | IDC(例) | DCIS(例) | 其他病变 | 恶性率(%) |
|---|---|---|---|---|---|
| 20~29岁 | 82 | 0 | 0 | 82 | 0.00 |
| 30~39岁 | 250 | 1 | 0 | 249 | 0.40 |
| 40~49岁 | 176 | 1 | 0 | 175 | 0.57 |
| 50~59岁 | 31 | 2 | 1 | 28 | 9.68a |
| 60~71岁 | 3 | 0 | 0 | 3 | 0.00 |
| 合计 | 542 | 4 | 1 | 537 | 0.92 |
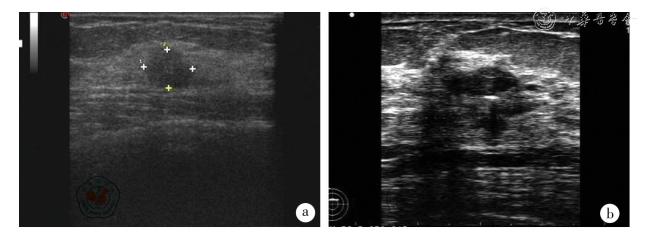
图1 2 例恶性病例术前超声图a:50 岁患者,超声示10.6 mm (横径)×8.5 mm (纵径)低回声占位,BI-RADS 3 级,病理检查示浸润性导管癌;b:55 岁患者,超声示10.87 mm(横径)×4.82 mm(纵径)低回声占位,BI-RADS 3 级,病理结果示浸润性导管癌。 |
表2 5 例恶性病例的临床资料 |
| 分组 | 恶性病例 | 平均年龄(岁) | 直径(cm) | 病理类型(例) | TNM分期(例) | ||
|---|---|---|---|---|---|---|---|
| DCIS | IDC | 0期 | Ⅰ期 | ||||
| 即时活检组 | 4 | 47 | 1.0 | 0 | 4 | 0 | 4 |
| 随访活检组 | 1 | 59 | 0.5 | 1 | 0 | 1 | 0 |
| [1] |
Mariotti C, Feliciotti F, Baldarelli M, et al. Digital stereotactic biopsies for nonpalpable breast lesion [J]. Surg Endosc,2003,17(6):911-917.
|
| [2] |
American College of Radiology. BI-RADS-US, American College of Radiology (ACR) Breast Imaging Reporting and Data System Atlas (BI-RADS Atlas). Reston,2003:77-79.
|
| [3] |
Meloni GB,Dessole S,Becchere MP,et al. Ultrasound-guided mammotome vacuum biopsy for the diagnosis of impalpable breast lesions [J].Ultrasound Obstet Gynecol,2001,18(5):520-524.
|
| [4] |
Hong AS, Rosen EL, Soo MS, et al. BI-RADS for sonography: positive and negative predictive values of sonographic features [J]. AJR Am J Roentgenol,2005,184(4):1260-1265.
|
| [5] |
Heinig J,Witteler R,Schmitz R,et al. Accuracy of classification of breast ultrasound findings based on criteria used for BIRADS [J]. Ultrasound Obstet Gynecol,2008,32(4):573-578.
|
| [6] |
Raza S, Chikarmane SA, Neilsen SS, et al. BI-RADS 3, 4, and 5 lesions: value of US in management follow-up and outcome [J]. Radiology,2008,248(3):773-781.
|
| [7] |
Costantini M, Belli P, Ierardi C, et al. Solid breast mass characterization: use of the sonographic BI-RADS classification [J]. Radiol Med,2007,112(6):877-894.
|
| [8] |
万舰,王永南,王颀,等.乳腺影像报告与数据系统在超声检查可扪及乳腺肿块中的诊断价值[J/CD].中华乳腺病杂志:电子版,2010,4(4):381-388.
|
| [9] |
Baum JK, Hanna LG, Acharyya S, et al. Use of BI-RADS 3-probably benign category in the American College of Radiology Imaging Network Digital Mammographic Imaging Screening Trial [J]. Radiology,2011,260(1):61-67.
|
| [10] |
Graf O, Helbich TH, Hopf G, et al. Probably benign breast masses at US: is follow-up an acceptable alternative to biopsy? [J]. Radiology,2007,244(1):87-93.
|
| [11] |
Yucesoy C, Oktay NA, Ozturk E, et al. Pathologic assessment of non-palpable probably benign breast masses at sonography: can instant intervention be avoided and is follow-up adequate? [J]. JBR-BTR,2010,93(5):242-246.
|
| [12] |
Moon HJ, Kim MJ,Kwak JY,et al. Malignant lesions initially categorized as probably benign breast lesions:retrospective review of ultrasonographic,clinical and pathologic characteristics [J]. Ultrasound Med Biol,2010,36(4):551-559.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}